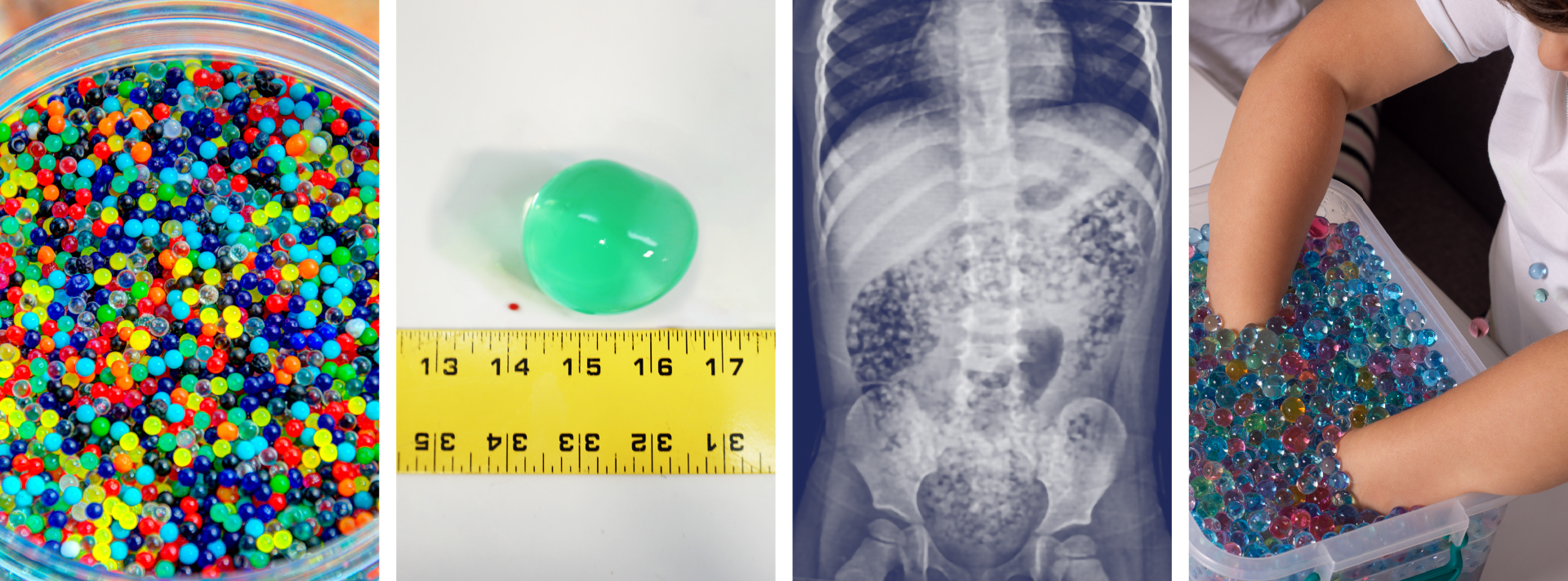
Water Bead
superabsorbent polymers, SAPs (Marketed as toys or decorative items)
Pharmacokinetics
SAPs are inert but expand physically. They are not metabolized, absorbed, or excreted. Their risk comes solely from swelling in liquid, which can block the GI tract.
Quick summary
- Presentation ranges from asymptomatic to vomiting, abdominal pain, decreased oral intake, or signs of bowel obstruction.
- Plain radiographs are often non-diagnostic; use ultrasound or CT if concern for obstruction and plain films are unrevealing.
- Management = risk stratify → imaging/observation → endoscopy if proximal and retrievable → surgical consult for obstruction/peritonitis.
Triage & initial assessment
- ABCs: airway patency (choking), oxygenation, hemodynamic stability. If airway compromise → immediate airway management.
- History: time of ingestion, estimated number/brand, bead size (pre-expanded vs hydrated), witnessed vs unwitnessed, symptoms.
- Exam: focused airway, chest, abdominal exam (tenderness, distention, bowel sounds), signs of peritonitis or sepsis.
- Baseline monitoring: cardiac, pulse oximetry, IV access, NPO if obstruction suspected.
Risk stratification
Higher risk
- Young infants or toddlers (<3 years) or any child with multiple beads ingested.
- Symptoms: persistent vomiting, severe abdominal pain, distention, inability to pass stool, peritonitic signs.
- Evidence of obstruction on imaging or clinical deterioration.
Lower risk
- Asymptomatic, single small bead ingested, short interval since ingestion, normal exam.
- Observed ingestion with beads already hydrated and passing without symptoms.
Investigations
- Plain radiograph (AP chest/abdomen): quick — but many beads are radiolucent; a normal x-ray does not exclude beads.
- Point-of-care ultrasound (POCUS): useful to visualize fluid-filled/anechoic spherical structures in GI tract and to follow progression; repeat as clinically indicated.
- CT abdomen/pelvis with IV contrast: consider if ultrasound equivocal and high suspicion of obstruction, ischemia, or perforation.
- Lab tests: BMP (for dehydration/electrolyte imbalance), CBC if concern for infection, lactate if ischemia suspected.
Management pathway (algorithm)
🚨 Red flags — require urgent surgical consult:
- Persistent vomiting with distention
- Severe abdominal pain or peritonitic signs
- Evidence of obstruction, ischemia, or perforation on imaging
- Clinical deterioration despite observation
-
Asymptomatic, low-risk patients:
- Educate caregiver; observe in ED 4–6 hours with serial abdominal exams.
- If remains well → discharge with clear return precautions and outpatient follow-up.
-
Symptomatic or higher-risk patients:
- Obtain POCUS ± CT to localize and assess size/clumping and obstruction signs.
- If bead(s) in esophagus/stomach and retrievable → consult GI/ENT for endoscopic removal.
- If beyond reach but no obstruction → admit for observation, serial exams, repeated imaging.
-
Obstruction, progressive distention, peritonitis, or failed conservative management:
- Urgent surgical consultation; prepare for operative intervention.
- Resuscitate with IV fluids/electrolytes; give broad-spectrum antibiotics if perforation suspected.
Special considerations
- Multiple beads: higher risk of conglomeration/bezoar formation.
- Airway foreign body: if aspirated → urgent ENT/bronchoscopy.
- Chemical toxicity: most are non-toxic, but mechanical obstruction risk is key.
- Documentation: record brand, quantity, time, symptoms, and imaging.
Disposition & follow-up
- Discharge if asymptomatic, normal exam, and reliable caregivers.
- Admit if symptomatic, multiple beads, abnormal imaging, or unreliable follow-up.
- Arrange GI/surgical follow-up if not retrieved or if ongoing GI symptoms.
Practical tips
- Use serial POCUS to track bead progression.
- Low threshold for surgical consultation in young children with multiple beads.
- Educate families — beads are candy-like and attractive to children.
